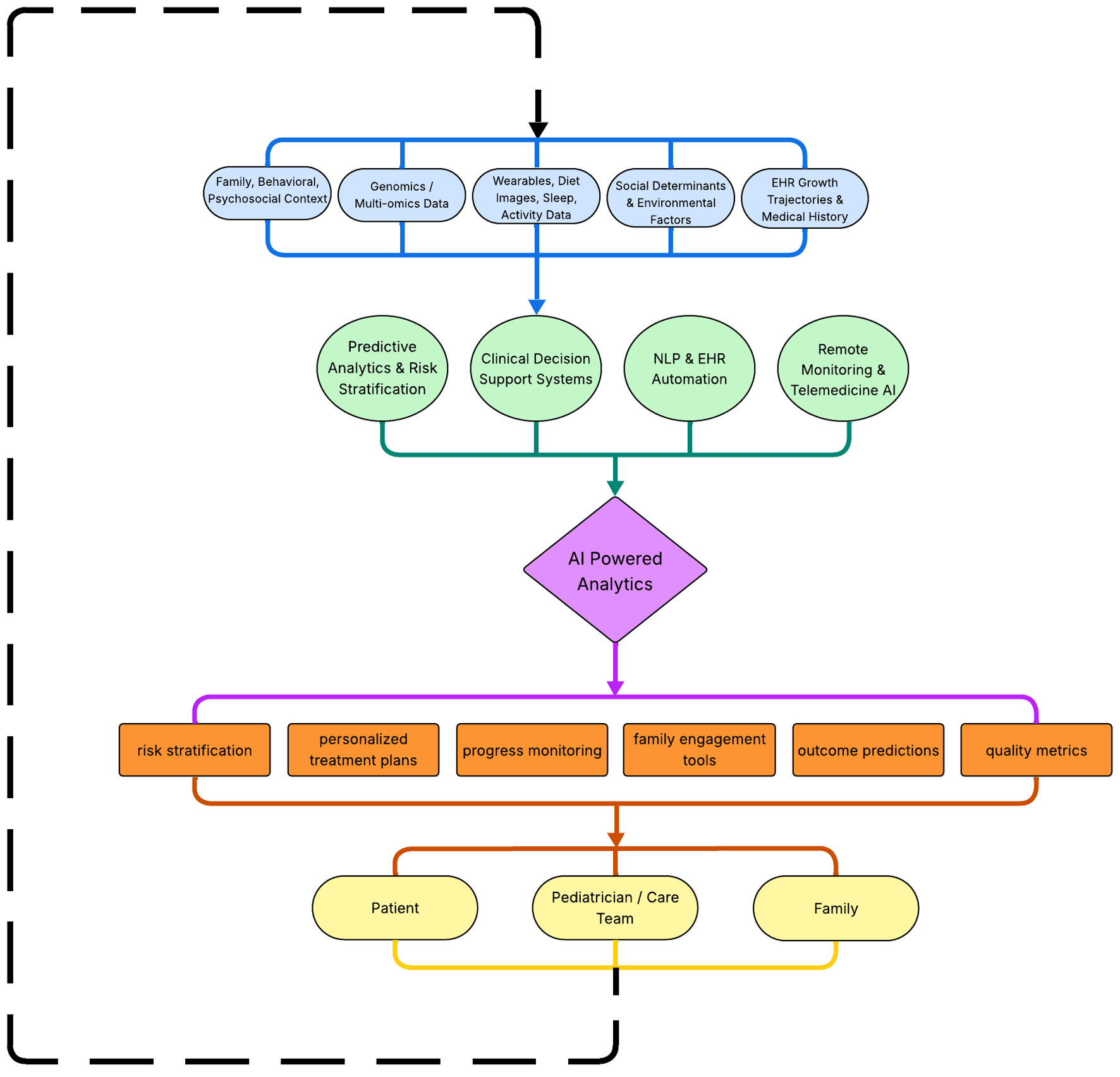
↓ Figure 1. AI workflow in pediatric obesity care pathway. The figure depicts the flow of various information types (e.g. medical records, wearable device data, family context, and environmental factors) into a single AI engine. This engine analyzes the aggregated data and provides insights and guidance to families, patients, and pediatric care teams. Actions taken by these groups generate new data, which are subsequently reintegrated into the AI engine, establishing a continuous feedback loop. Source: Figure created by authors JP, MS, and VSC using Microsoft PowerPoint from data extracted from sources [16–20]. AI: artificial intelligence.